
cath lab display screens factory
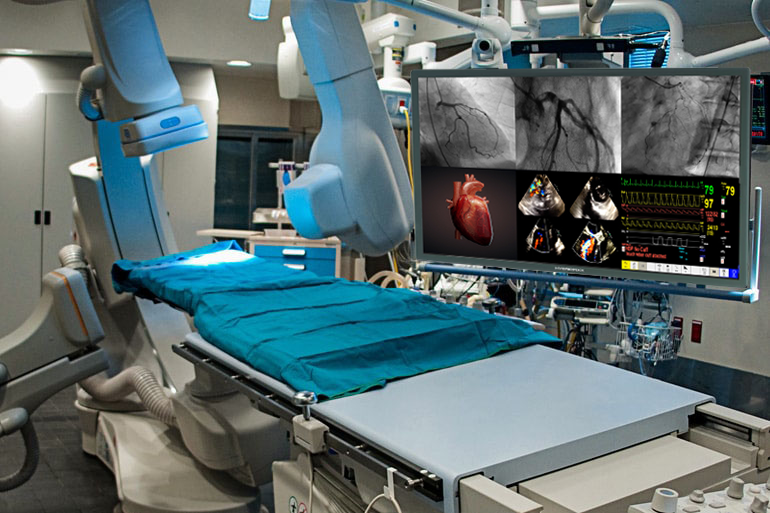
Cardiac Cath Lab display monitors such as the Modalixx offer a multi-modality approach which sanctions the exhibition of a wider range of imagery and promotes efficient work flow. The constant advances in medical imaging technology called for upgraded systems from old CRT monitors, these auto-sync devices are produced to combat this issue. Compatible with a multitude of well-known manufacturers such as GE, Siemens, Toshiba, Shimadzu, Philips and other modalities, Ampronix is constantly working to offer imaging solutions for all display and peripheral needs in the medical field.

We have been Repairing & Selling 4K monitor’s sized 56”, 58”, & 60” for Cath Labs, & Hybrid OR’s to hospitals for years and wanted to make sure you are aware of our capabilities.
The next breakthrough in medical technology stems from ultra-high definition LED monitors with the capability of displaying imagery at 4K / 8MP with 3840 X 2160 resolution adept for multiple application viewing on a single screen. These monitors make existing CRT/LCD displays a thing of the past for Cath Lab and Hybrid OR facilities. Ampronix offers service, repair, and replacement of all 4K systems including large screen displays, hybrid monitors, and consumer displays. The onsite, full service and repair warehouse is composed of a dedicated team of experts working on the repair and maintenance of top brands such as Eizo, Barco, Optik View, and HYBRIDPIXX to reestablish factory standards.
Ampronix maintains and quickly repairs all 4k medical display monitors to ensure no time is lost in situations of criticality. There is nothing as vital as imaging equipment in a Cath Lab or Hybrid OR, in a medical procedure up to 4-6 monitors can be utilized at a time for enhanced visibility. These UHD large medical grade displays are considered to be the new “gold standard” for surgical applications allowing multiple screens to be viewed on a single device while taking up a minimal amount of space.
This video manager box, included with the purchase of an Ampronix 4K Hybrid display, allows compatibility between existing Cath Lab modalities and higher resolution displays. This proves advantageous for customers looking to avoid high costs of replacing an entire system that needs to upgrade a modality"s interface.
If a Cath Lab modality with 2K cable outputs cannot properly read monitor inputs, the 4KBoxx22 works as an emulator, reestablishing system communication to the display. However, in instances where the Cath Lab has four 1K cables, the 4KBoxx 422 will convert them into two 2K cables before emulating signal. This ensures that the Cath Lab has the capacity to transmit to the intended display. Click here to learn about how the 4KBoxx is used in application.

If you’re involved with managing a Cath Lab have you had your physicians ask to upgrade to a newer digital interventional x-ray system or add high-definition digital large flat screen monitor displays? When planning a remodeling project or lab expansion it is important to have the latest in imaging technology. In order to keep cardiologists happy, or recruit new physicians, hospitals need to be competitive in the local market and provide the newest and highest-quality digital imaging.
But the process to upgrade an x-ray system or add a new lab suite can take time. Starting with budgeting, waiting for funding, approvals, PO’s, and construction schedules it can take anywhere from a few months to a few years to complete.
We’re aware of these challenges and for over 30 years Modular Devices Inc. has offered solutions to lab upgrade and expansions with our interim Mobile Cath Lab and Modular Cath Labs. Our interim Cath and Vascular Lab systems can be quickly and easily brought in and parked at a hospital to provide support on either a short (month-to-month) or long-term basis. Our labs are equipped with the latest digital flat panel detector cardiac/interventional imaging systems, offering an effective way to provide your physicians with newer x-ray imaging technology in the interim while plans are being made to upgrade the in-house lab to new equipment.
In order to properly maintain our fleet of 26 interim labs we’re continually updating the x-ray systems and making other improvements to keep them up to date with the latest technology.
Always listening to our customer’s feedback and reviews we’re very excited to announce the most recent update to our interim lab fleet – large flat screen monitor displays. These high-definition large flat screen monitors measure between 50″-58″ and replace the typical display setup mobile Cath Labs which includes a ceiling-mounted boom with 3 LCD displays (live, reference and hemodynamic monitoring).
In the past we could add additional monitors to the boom for clients who utilize an IVUS system or for 3D EP imaging, for example, but with the large flat screen monitor displays the inputs can be be displayed and rearranged on different sections of the large flat screen display.
This new product roll-out is the perfect solution for long or indefinite term Modular Cath Lab projects where physicians require a large screen monitor in an interim Cath Lab now while they wait for the new lab construction project to be completed down the road.
If you’re interested in learning more about our Mobile and Modular Cath, Vascular Lab solutions can help with a lab renovation or expansion – give us a call at 800-456-3369 or click here to Contact Us.

The Double Black Imaging FP4204B-MED large screen LCD is a medical grade display certified to EN/UL 60601 safety requirements for patient vicinity use. It features a unique, acrylic protective panel integrated and sealed into the bezel (IPX1-rated), which protects the screen and enables proper wipe-down and cleaning protocol.This 42” display utilizes full 1920 × 1080 HD resolution (2MP) and provides bright, clear images.
DBI’s FP4204B-MED display accepts a variety of input signals, including DP, DVI-D, HDMI, VGA, CVBS, and S-Video. Mount the display in almost any location, including for PACS analysis in the OR, with no risk of compromising image quality. Options are available for fixed or articulated wall mounting or cart mounting. Alternatively, position the display for use with a PC or workstation.
The protective panel also guards against unintentional physical contact, maximizing each display’s long-term performance without compromising image quality. The panel’s anti-reflection surface also limits the glare of bright operating room lights.
Each Double Black Imaging FP4204B-MED display comes with a 1 year warranty and exceptional support from the Double Black Imaging team of knowledgeable engineers and technicians to ensure that images are consistent and accurate for critical medical applications.

This GE Innova 3100 IQ Cath Lab has been completely refurbished from the ground up to factory specifications. This lab is unique as it has a 2014 X Ray Tube plus a 2015 60′ Flat Detector.

After connecting the IntelliVue X3 to its docking station at the tableside of the Azurion system, clinical staff can monitor all of the patient’s vital signs including pulse oximetry end-tidal CO2, perform hemodynamic analyses and 12-lead ECG acquisitions, and relay results and waveforms from the lab’s control room to the Azurion tableside display. From the tableside the interventionalists can assess the data using the Azurion tableside Touch Screen Module, allowing them to remain focused on their patients. The system brings the latest physiological techniques to the interventional lab, including iFR (instant wave-Free Ratio) measurements, a hyperemia-free technique unique to Philips that provides valuable functional information regarding the severity of lesions in the coronary arteries.
Philips Interventional Hemodynamic System with Patient Monitor IntelliVue X3 integrates with Azurion, the company’s next-generation image-guided therapy system that allows clinicians to easily and confidently perform procedures with a unique user experience, helping to optimize lab performance and provide superior care. At ACC.21 Philips will showcase its solutions for the diagnosis and treatment of Structural Heart Disease, which aim to remove the barriers associated with complex procedures by helping to deliver clinical confidence where it is needed most – at the point of treatment. Philips’ cardiac care solutions help strengthen clinical confidence, build efficiency throughout the care pathway, and enhance care experiences. For more information visit www.philips.com/acc.
[1] Philips Interventional Hemodynamic System with Patient Monitor IntelliVue X3 is available in the majority of markets worldwide. Philips’ continuous patient monitoring solution is available for sale in markets across Europe, Middle East and APAC, with further expansion planned later this year. It is not available for sale in the U.S.

Although the imaging machines surgeons typically use to peer into the body collect data in three dimensions, the images are displayed on two-dimensional screens. That means surgeons doing minimally invasive procedures have no depth perception and need to periodically tap internal surfaces to get oriented.
“We developed the method of real-time streaming of (ultrasound) data into head-mounted mixed-reality holographic display allowing for touchless control and data sharing within the cath-lab,” the research team led by Jaroslaw Kasprzak, a cardiologist at Bieganski Hospital and chair in the department of cardiology at the Medical University of Lodz writes. “The method was tested for the first time in a human during (a procedure to widen the mitral valve).”
During that procedure, a deflated balloon is placed inside the narrowed valve and then inflated to widen the opening so blood will flow more freely, explained Dr. Omar Ali, director of the cardiac catheterization lab at Detroit Medical Center’s Heart Hospital in Michigan. Ali was not involved with the new research.
“3D holographic displays such as the one mentioned have the potential to allow operators to utilize this valuable information and modify techniques in real time, permitting dynamic guidance during an ongoing procedure,” Bazaz, a cardiac electrophysiologist with the Heart and Vascular Institute at the University of Pittsburgh Medical Center said in an email. “The synthesis of computation and real-time imaging hold promise to permit more optimal outcomes than attainable in the past.”

1Prasad A, et al. Contemporary trend of acute kidney injury incidence and incremental costs among US patients undergoing percutaneous coronary procedures. Catheter Cardiovasc Interv. 2020 Nov;96(6):1184-1197.
2Castro D, Dang TT. Reducing contrast-induced acute kidney injury in the cath lab. Poster presentation at ACC National Cardiovascular Data Registry (NCDR) 2018 Annual Conference.
3Thukral N. Kidney care protocols in the cath lab. Transcatheter Cardiovascular Therapeutics 2019 Presentation. Accessed on October 14, 2019 from: https://www.tctmd.com/slide/aki-reduction-cath-lab-protocol-development-implementation-and-outcomes.
4Turner C, Tucker PA. Real-world impact of a quality improvement program for AKI prevention in the cardiac cath lab. SCAI Scientific Sessions Virtual Conference. Catheter & Cardiovasc Interv. 2020;95 (Supplement 2): S112-S113.
5Cameron A, Espinosa TJ. Reducing contrast-induced acute kidney injury in a cardiac catherization laboratory: a quality improvement initiative. SCAIScientificSessionsVirtualConference. Catheter&CardiovascInterv. 2020;95(Supplement 2):S25.
8Sattar A, et al. Impact of using DyeVert Plus on incidence of acute kidney injury after cardiac catheterizations with coronary interventions in high risk patients. ACC Annual Meeting 2018; Charleston, WV.
9Briguori C, Golino M, Porchetta N, et al. Impact of a contrast media volume control device on acute kidney injury rate in patients with acute coronary syndrome. Catheter & Cardiovasc Interv. 2020 Jul 18. doi: 10.1002/ccd.29136.
Three times in as many months, the computerized systems at the heart of Stanford University Medical Center’s cardiac catheterization labs froze, locking up tighter than a plaque-clogged artery. Mark Addis, CBET, of the clinical technology and biomedical engineering department needed to figure out the reason why.
Soon enough, he had his answer: the information technology (IT) department had been loading third-party anti-virus software at a data center server farm, and this software was incompatible with the proprietary programming package running on the networked systems in the cardiac cath labs. “Every time IT did this, it chewed up nearly all the RAM in my systems’ CPUs, which disrupted all 12 of the labs at the same time,” Addis says, whose main responsibility at the Palo Alto, Calif, hospital is the care and feeding of those rooms.
The first step Addis took to solve the problem was convince hospital decision-makers to give the cath labs a network domain of their own, one that he would control despite it still being on the IT department’s network. Equally important, he created a five-page document containing spreadsheets and schematics of the network interfaces with his systems. “I’ve got all the static addresses, including port locations and individual serial numbers,” he says. “So, now, if I am unable to ping any system on the cath lab network or if a networked system is running slow, I look up the name of the most appropriate IT person and give him or her the IP address of the system that’s in trouble, then ask if they can help me diagnose and repair the network problem.”
Cardiac cath labs have been around since at least the 1960s, and there is not a major hospital anywhere in the nation without one—or two, or three, or more. Still, some institutions are only now getting around to bringing them aboard. “Mostly these are smaller facilities where this is happening,” says Craig Williams, CRES, recently retired senior field service specialist at Centura Health St Anthony’s Hospital in Denver and Westminster, Colo.
A cardiac catheterization laboratory is a room designed for the diagnosis and treatment of various conditions of the human cardiovascular system. For example, cardiac catheterization is considered the definitive test for the detection of coronary artery disease, the leading killer of adults of both sexes in the United States. Procedures almost invariably involve the insertion of a catheter into an artery of the patient’s arm or leg. The catheter is then guided along the artery until it reaches the heart. A variety of instruments—probes, cameras, wires, borers, cutters, or balloons—can be passed through the catheter to access whatever lies on the opposite end. All of this is accomplished using some rather sophisticated systems, starting with a hemodynamic monitor to keep tabs on the patient’s blood pressure and electrocardiogram data during procedures.
“Here at Stanford Hospital, each of our 12 rooms has hemodynamics equipment, primarily the MACLAB IT from GE,” Addis says. “Each hemodynamic unit consists of a computer, an integrated electronic box providing power and video to multiple monitors, and a TRAM module for collecting patient ECG, NIBP, invasive blood pressure, temperature, and SP02 data. There is also an EtC02 module for collecting patient C02 and respiratory rate data, a real-time display monitor and a review display monitor at the control workstation, and a real-time monitor at the procedure table.”
Some cath labs augment hemodynamic monitoring by adding an electrophysiologic monitor to look at patient intracardiac electrical activity and surface ECGs. “The electrophysiology system we’ve installed in four of our cath labs receives NIBP, SP02, EtC02, and temperature from the hemodynamics system, but adds a CardioLab amplifier to collect patient ECGs, invasive pressures, intercardiac signals, and cardiac stims,” Addis says. “The addition of electrophysiology capability also adds a third monitor at the workstation to collect fluoroscopy images and a review monitor at the procedure table.”
The fluoroscopy images to which he refers are generated by the single-plane or biplane x-ray system that every cardiac cath lab must install in order to safely guide the catheter on its journey through the artery. “The imaging systems in our cath labs are mostly Siemens, but we also have one from Philips and two, soon to be three, from GE,” Addis offers. It is not uncommon to find alongside the x-ray system an ultrasound scanner. This is typically employed to locate peripheral arteries. Nor is it unusual to find a more specialized ultrasound unit called an intravascular ultrasound system that produces images from inside the artery or heart rather than from outside.
Lasers too show up in cardiac cath labs. “We have a Spectranetics CVX-300 for, among other things, peripheral atherectomy and coronary atherectomy, and an AngioDynamics ELVS for treatment of severe varicose veins,” Addis says. “Our equipment complement is rounded out by a device called a Rotablator from Heart Technology that removes coronary artery blockages. It does this with a diamond-coated burr that spins up to 190,000 RPM inside the artery, converting plaque into particles smaller than red blood cells so that the body can remove the plaque as normal waste.”
Service issues associated with these various pieces of equipment run the gamut from simple to the vexing. For Williams, whose responsibilities at the two Colorado hospitals where he worked were three cath labs, an electrophysiology lab, a room for the programming of pacemakers, and nine prep suites, it was the hemodynamic systems that consumed the largest share of his time, but not due to equipment reliability.
“The problem was we had nontechnical personnel interfacing with a highly technical application,” Williams says. “The users of the hemodynamic system sometimes had difficulty understanding its capabilities and limitations, so a big part of my job was providing guidance to the clinical staff. For example, I would get a call for help from the electrophysiology lab; I would show up, ask what seemed to be the trouble, and the staff would spell out how this or that was all out of whack. I would then ask a few pointed questions, the invisible light bulb would turn on over their heads, and it would dawn on them what they needed to do in order to fix it themselves.”
That is not to suggest that cath lab systems are themselves trouble-free. Take hard drives. They, of course, sometimes go down. To minimize the effects of failed storage devices, Williams made a point of cloning each hemodynamic system’s computer hard drive every time he performed preventive maintenance (PM). “If a system died and the cath lab was down because of it, rather than spend 2 or 3 days replacing the computer, I simply grabbed the clone of its hard drive from where it was kept in my office, plugged it in, and could have the system booted back up in minutes,” he says.
Being a former factory field engineer and the beneficiary of extensive subsequent training, Williams was able to fully service his hospital’s hemodynamic systems on his own. Only the lab’s x-ray systems were under service contract—and a shared one, at that. “The reason for the shared arrangement was to ensure that we could quickly obtain the parts we needed,” he says. “That was important because these x-ray systems are so parts-intensive. Also, the service contract guaranteed coverage during the times I was off on vacation or out due to illness.”
The PM process at St Anthony’s entailed twice-annual inspections of the x-ray and hemodynamic systems, a process that consumed 1 full day per piece of equipment. Says Williams, “With the x-ray system, we conducted basic checks for radiation safety, calibration, and image quality. For the hemodynamic system, we confirmed that all ports were reading, that all displays were proper, and that pressures were accurately calibrated.” Tools Williams carted in on PM day included a laptop computer, a memory stick, a dosimetry gauge, and the usual assortment of screwdrivers, sockets, wrenches, and the like. The amount of time needed to PM each system necessitated careful coordination with the cath lab staff. “If a room was to be PM’ed, we had to schedule it well in advance,” Williams recounts. However, scheduling was no guarantee the room would be available to him for the full day. “I had to be ready to clear out at a moment’s notice and restore the room to full functioning. That’s because you can’t tell the cardiologist, sorry, but your emergency patient who’s dying can’t be in the room because I’ve scheduled it for PM.”
In the event Williams had to halt a PM in midcourse, he rescheduled it for another day. “The challenge in that was the cath labs were my highest priority, so any other work calendared for the same day of the rescheduled cath lab PM had to itself be rescheduled.” The resultant ripple effect could prove maddening.
Electronic noise is a big issue for biomeds in their care and feeding of cardiac cath labs. “Sixty-cycle noise interferes with the ability of the lab team in the electrophysiology rooms to detect certain heart conditions, such as tachycardia and other arrhythmia,” Addis says. “As a result, a signal must be as clean as possible, which means monitor cables have to be properly maintained. If I find frayed, worn, or broken cables, I replace them immediately.” And wear out they do, especially ECG surface lead cables. “These are radiotranslucent, so that they do not appear on the fluoro images, but their phenolic grabbers deteriorate quickly. I make it a point to change these radiotranslucent leads approximately every 3 months. The hemodynamic systems also have them, but don’t wear out as fast, so I space the replacement frequency to once a year.”
Addis finds that some seemingly minor PM chores can in reality be mission-critical. Checking the computer cooling fan grilles on the hemodynamic systems is a good illustration of how this is so. “Patient linen is washed and sterilized after each use, which gives off lint in the lab,” he says. “Enough lint is given off that the fan grilles can become completely clogged with it. As a result, when I perform my PM on the systems, I bring a HEPA-filter vacuum to give the computer a really thorough cleanout.”
In a sense, that is much akin to what transpires in the lab itself when patients are present. Making sure the equipment is able to clean out the arteries when the physicians and nurses go to use those systems is what the biomed contribution to the cardiac catheterization lab is all about.
The term “catheterization lab” is sometimes used when referring to a similar but not entirely identical room known as a “vascular lab.” As a result, each can be confused with the other.
“Technically, a cardiac cath lab is a vascular lab, and they both do the same kind of work with many of the same kinds of systems and devices, but the difference is that the vascular lab does not concern itself with the heart, while the cardiac cath lab does,” says Craig Williams, CRES, recently retired senior field service specialist for Centura Health St Anthony’s Hospital in Denver and Westminster, Colo.
Contributing to the confusion is a blurring of turf barriers. “The cardiac cath lab is operated by the department of cardiology, while the vascular lab is operated by the department of radiology,” Williams indicates. This division seems straightforward enough, until the cardiologist brings in a patient with vascular disease of the heart. “If the patient has vascular disease in the heart, it’s likely he has vascular disease elsewhere in the body, particularly the legs,” Williams continues. “The cardiologist says he can handle the whole case himself in his cardiac cath lab, so why bother sending the patient to the vascular lab? And the opposite is true of radiologists with their vascular patients.”
What is beginning to happen as a result is a tight pairing of the two fields within the confines of the cath lab. Case in point: at St Anthony’s, the three newest cath labs are all dual-purpose rooms, able to handle both coronary and vascular cases.
Long ago, cardiac cath labs and vascular labs were easier to tell apart by the equipment they utilized. “Vascular labs had film changers along with photo-spot cameras that could run to four or six frames per second, while the cardiac cath lab utilized cameras capable of speeds of 30 and 60 frames per second,” Williams says. “Today, the systems employed in the cardiac and vascular labs are different only in detector size and software features.”

Administrative Offices Anesthesia Bio Med Storage Business Office C Section Cardiology/ EEG/ EKG/ Stress Storage Cath Lab Central Supply Clean Linen Clean Supply/Clean Utility Clean Utility Cystoscopy Dining / Kitchen Emergency Department Employee Lounge Endoscopy EVS/Housekeeping Eye Clinic Gift Shop / Volunteer Storage ICU Infection Control Information Technology Isolation Labor & Delivery/PICU/NICU/C-Section Laboratory LTC Maintenance / Engineering Materials Management Medical Records Medication Room Nurses Station Nursing Floor Storage Opthamology Outpatient Surgery / Ambulatory Surgery Centers Patient Dressing Rooms Pediatrics Pharmacy Physical Therapy Physician"s Lounge Point of Use Radiology Respiratory Therapy Soiled Utility Surgery/OR Storage/SPD Storage Warehouse

For patients needing emergency cardiac catheterizations, we hold the distinction of maintaining a "door-to-balloon time" of under 70 minutes. This means that, from the time you enter our doors, the catheterization begins within 70 minutes. This is faster than the national standard of 90 minutes that is recommended by the American College of Cardiology and the American Heart Association.
We perform many of these advanced procedures in the largest catheterization labs on Long Island, all fully equipped with the latest in diagnostic and interventional medical devices. We were also the first New York State Department of Health-approved laboratory on the south shore of Nassau County.
Using advanced tools and techniques, we diagnose and treat blocked arteries. For example, to diagnose blockages and develop a treatment plan, the GE fluoroscope is one of the most technologically advanced diagnostic tools available. It allows our physicians to view the inside of the heart vessels in real time using sound waves (intravascular ultrasound), to evaluate the blood supply to the heart. This test offers the most accurate diagnosis of a blockage in the artery, and precision in placing a stent. It also gives high-tech measurements of how much pressure is being exerted on the blood vessel, which our physicians also use to determine the most appropriate treatments.
Balloon angioplasty is the most common of our treatments for blocked blood vessels. During this procedure, your surgeon threads a catheter with an inflatable balloon into an artery and guides it to the blockage. The surgeon then inflates a tiny balloon inside the catheter, which pushes plaque against the artery wall, allowing blood to flow normally. We often use stents, as well, to keep the artery open.
Rosenberg’s wife, Janie, called an ambulance that took him to Mount Sinai South Nassau’s Emergency Department, where staff quickly diagnosed him with acute myocardial infarction: a heart attack. His heart muscle was being starved of oxygen. But Dr. Jason Freeman, Director of Interventional Cardiology, also acted quickly. He performed an angioplasty to open Rosenberg’s blocked coronary artery using a balloon-tipped catheter.

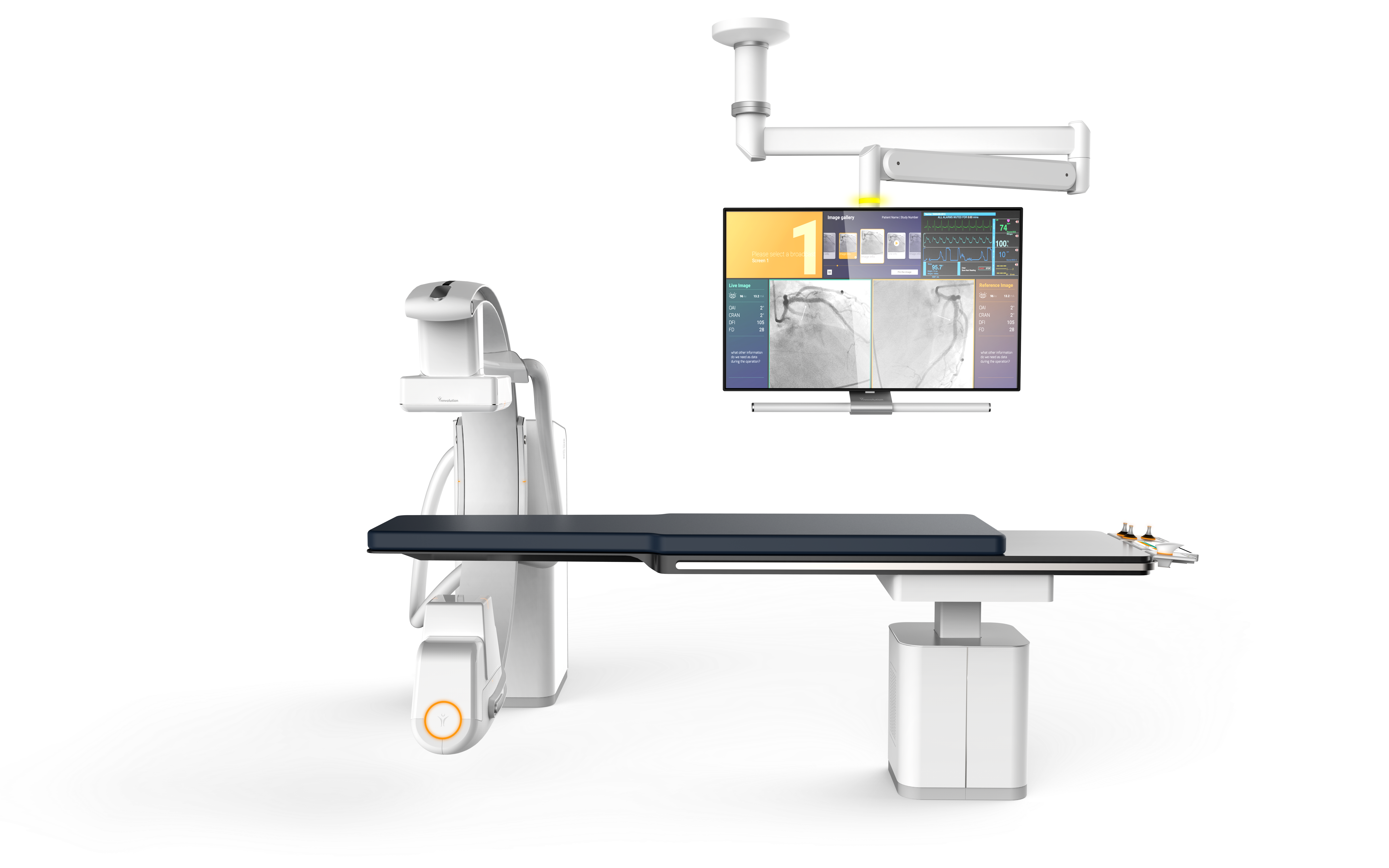
Setting up a cath lab with all the right options for your specialty, your workflow, and your physicians" preferences comes with a lot of questions. Among those we"re asked most often: How many monitors come with a cath lab system?
The answer to that question isn"t 100% cut-and-dry, but we can help you know what to expect as you begin shopping. Keep reading to learn more about monitor options for your next cath lab system.
Typically, cath labs come with just 2 monitors included on the monitor suspension arm: a live monitor, and a reference monitor. Seems like an easy enough answer, right?
The extra positions on the monitor suspension are for, you guessed it, extra monitors! Okay, that’s a bit of an over-simplification, so let us explain. In the cath lab, more than any other modality, peripheral systems are used to help treat the patient. Depending on what these systems are and how many you have, it may be preferable to add one, two, or even six more monitors onto your suspension.
Most cath labs use a hemodynamic monitoring system such as a GE MacLabduring studies. There is often a monitor on the suspension that displays the patient"s physio data in real time so the staff has immediate feedback from the MacLab.
If you’re in a lab that performs 3D studies, there is a good chance the cath lab itself is unable to reconstruct the raw data acquired during a study. In this case, a reconstruction workstation such as a GE Advantage Windows Workstation (AWW) is needed to reconstruct the images. When a reconstruction workstation is in use, one of the monitor slots on the suspension can be dedicated to displaying reconstructed image data.
When a site orders a new cath lab from the manufacturer the number of spaces available on the monitor suspension can be selected. If you plan to purchase your lab on the secondary market, be sure to talk to your provider early on about how many monitor spaces you"ll need so they can accommodate. For single-plane labs, suspension systems are available with two to six monitor spaces. Suspensions for up to eight monitors are available for biplane systems.
If you have additional questions about monitors or monitor suspensions, are in need of a cath lab, or need some peripheral equipment to help fill out your monitor suspension, call or email us today



 Ms.Josey
Ms.Josey 
 Ms.Josey
Ms.Josey