
cath lab display screens in stock
Setting up a cath lab with all the right options for your specialty, your workflow, and your physicians" preferences comes with a lot of questions. Among those we"re asked most often: How many monitors come with a cath lab system?
The answer to that question isn"t 100% cut-and-dry, but we can help you know what to expect as you begin shopping. Keep reading to learn more about monitor options for your next cath lab system.
Typically, cath labs come with just 2 monitors included on the monitor suspension arm: a live monitor, and a reference monitor. Seems like an easy enough answer, right?
The extra positions on the monitor suspension are for, you guessed it, extra monitors! Okay, that’s a bit of an over-simplification, so let us explain. In the cath lab, more than any other modality, peripheral systems are used to help treat the patient. Depending on what these systems are and how many you have, it may be preferable to add one, two, or even six more monitors onto your suspension.
Most cath labs use a hemodynamic monitoring system such as a GE MacLabduring studies. There is often a monitor on the suspension that displays the patient"s physio data in real time so the staff has immediate feedback from the MacLab.
If you’re in a lab that performs 3D studies, there is a good chance the cath lab itself is unable to reconstruct the raw data acquired during a study. In this case, a reconstruction workstation such as a GE Advantage Windows Workstation (AWW) is needed to reconstruct the images. When a reconstruction workstation is in use, one of the monitor slots on the suspension can be dedicated to displaying reconstructed image data.
When a site orders a new cath lab from the manufacturer the number of spaces available on the monitor suspension can be selected. If you plan to purchase your lab on the secondary market, be sure to talk to your provider early on about how many monitor spaces you"ll need so they can accommodate. For single-plane labs, suspension systems are available with two to six monitor spaces. Suspensions for up to eight monitors are available for biplane systems.
If you have additional questions about monitors or monitor suspensions, are in need of a cath lab, or need some peripheral equipment to help fill out your monitor suspension, call or email us today

Modular Devices offers short and long-term interim rentals of temporary Mobile and Modular Cardiac Cath, Peripheral Vascular, Electrophysiology (EP) and CT Labs to hospitals and healthcare facilities throughout the USA and North America. Reflecting our commitment to high-quality standards, every lab in our fleet is fitted with only the newest and most advanced imaging technology available.

Our cath lab team consists of 2 interventional cardiologists, 4 registered nurses (RNs), and 2 radiologic technologists (RTs). One of the nurses currently holds the registered cardiovascular invasive specialist (RCIS) credential, one RT is studying for her RT(CI), and the second RT is RT(R)(M)(ARDMS). Each team member is currently making strides to gain further certification and/or education to enhance patient outcomes. Each of the team members currently performs at least two of the three roles of the cath lab team (monitor, circulating nurse, and scrub). The cath lab team started in January of 2013, but our cath lab and cardiology team member experience ranges from two years to 28 years. Our Big Horn Heart Clinic team consists of one office manager who is a respiratory therapist, two full-time RNs and one part-time RN, one echocardiographer, two schedulers, and one records person. Staff clinical and cardiac experience ranges from one year to 29 years.
Since we opened two years ago in January of 2013, we have performed 165 diagnostic cases, 67 interventional cases (not including STEMI), 21 STEMIs, 54 implants, 52 DCCV/TEEs, and 2 pericardiocentesis cases. This is significantly above the original projections for the cath lab, and we are gaining speed.
Each member of our team is cross-trained in at least two of the three positions in the cath lab. The RNs all circulate and then either scrub or monitor. The two RTs are cross-trained in monitoring and scrubbing. The team also performs various duties outside of the procedure room related to performance, including quality assurance/performance improvement measures, marketing, hospital employee education, and community awareness projects.
Which personnel can operate the x-ray equipment (position the image intensifier [II], pan the table, change angles, step on the fluoro pedal) in your cath lab?
The cath lab members that have been trained and show proficiency in operating the c-arm can position the II, pan and change angles; however, at this time, only the cardiologist/radiologist steps on the fluoro pedal.
Since the SMH Cath Lab opened in 2013, everything in the lab is new. We have an Artis zee floor-mounted system (Siemens) in the cath lab and an Artis zee ceiling-mounted system in the IR lab, with integrated fractional flow reserve (FFR)/intravascular ultrasound (IVUS) (Volcano Corporation). Our power injector is a Mark 7 Arterion (Medrad), and we have the AutoCAT2 WAVE intra-aortic balloon pumps (Arrow International). Our main PCI vendor is Abbott (we use the Xience stent), but we have supplies from many vendors. We have the Jostent Graftmaster (Abbott) available for our bailout system. We also have the AngioJet (Boston Scientific) for thrombectomy in the IR lab.
All cath lab staff has gone through training and is checked off yearly for proficiency in pulling sheaths. Both RNs and RTs are expected to pull both diagnostic and interventional sheaths per cardiologist orders. The ICU is currently starting training and proficiency check-offs for sheath pulling.
Patients with elective cases are brought to the ICU for prep of their heart cath. Post procedure, the heart cath patients return to the same ICU room for post-op care. Being able to see the same staff take care of them throughout their hospital/cath experience gives the patient quality continuity of care.
Our inventory is managed in a coordinated effort between the cath lab team and materials management team through Pyxis systems and Keane electronic ordering. We have a certified purchasing agent that is dedicated to ensuring best pricing for the cath lab department.
Can you share your lab’s average door-to-balloon (D2B) times and some of the ways employees at your facility have worked together to keep D2B times low?
Our institutional outcomes report through the National Cardiovascular Data Registry (NCDR) just came out last month, and gave us a rolling four-quarter D2B time of 59 minutes. We feel that this is an outstanding endeavor, considering that our new cath lab was opened from scratch just two years ago.
We have been working in a joint effort with local emergency medical services (EMS) and the hospital’s emergency and ICU departments to ensure best patient outcomes, including a 90-minute D2B on all STEMI patients. We use a group paging system to activate the entire cath lab at once. We have members of both the EMS and the hospital that are very active in the American Heart Association (AHA) Mission: Lifeline Wyoming (M:L/WY) initiative and committees, and use many of the tools that have been a product of the committees with M:L/WY, including the use of a STEMI guideline and checklist in the emergency department (ED). Our cath lab and ED have recently been added to the AHA M:L sites.
Due to the cath lab’s close proximity to the ED, all STEMI patients are being transported from the emergency department to the cath lab by the cardiologist and circulating RN. This transport time, from wheels up to wheels down, is typically around two minutes.
We have two scenarios available for our team if there is currently a patient on the table, and a STEMI arrives to the ED. Our first option is: if our second cardiologist is available and the second cath lab/IR lab is open, we assemble our second cath lab team, and perform the STEMI in our second lab. It is well furnished with the same items as the dedicated STEMI room.
If we only have one cardiologist available, and the cath lab/IR room is in use, then we will stabilize the case in progress, transport them to the ICU for observation, and turn the room around for the STEMI patient. Again, the second cath lab team is assembled, and prepares the room for an emergent case.
The hospital as a whole has tried to be very competitive in pricing. We have done this by being very lean in our pricing structure. The cath lab and materials management departments have also taken measures to account for waste, including comparing the cost of disposable supplies versus the use of sterile processing and reusable supplies, as well as dropped and contaminated supplies. Finally, our certified purchasing agent focuses on best pricing options through our two group purchasing organizations (GPO), Novation and MSS. We have also been able to consign most of our products, and have close relations with our vendors to rotate products out that have a six-month or less expiration date. Finally, one creative way that has helped cut costs to the hospital as a whole has been in integrating the cath lab team into IR department procedures. Due to the low volume of the lab, both RNs and RTs will assist in other cardiac and interventional areas of the hospital to help with echocardiograms, sedation, monitoring and scrubbing. This helps the hospital cut costs in wages (i.e. not bringing in large volumes of travelers), and helps the team stay proficient in their various skills (echo, IV starts, port accessing, lab draws, moderate sedation and recovery, and ambulatory clinic assessments).
We have two RNs and one RT dedicated to collecting data and monitoring trends within the cath lab environment. We specifically look at D2B for STEMI, contrast and fluoro usage per case and per physician, complications ranked by the NCDR, patients being transferred for coronary artery bypass surgery (CABG), and a new moderate sedation tool to ensure adherence to policy.
Fluoro times and dosages are recorded by the Sensis (Siemens) hemodynamic monitoring system, electronically sent to our final cath lab report, and transcribed into the final physician dictation.
Medications given in the cath lab procedures are documented by the monitor role during cases. To ensure that there is understanding, we use a “call-back” style of communication, as discussed in TeamSTEPPS (www.ahrq.org). This simply means that when a medication is given, the nurse calls out, for example, “1mg of Versed”, and the monitor person responds by stating, “Heard” or “1mg Versed”. This concept of communication started because the monitor person was separated by a lead window, and wasn’t always hearing the advancement of the procedure or medications given. It has decreased the amount of documentation errors.
Like most of Wyoming, Sheridan is very remote to most other facilities and cath labs in the state. Up until July 2014, Sheridan was only the third cath lab in the state. With our partnership with AHA’s Mission: Lifeline Wyoming, we have continued and strengthened our relationships with the regional medical centers in our state, as well as in Montana. Since we are a non-cardiovascular surgical PCI center, we must always keep open communication with our partnering cardiovascular surgical centers.
New employees to the cath lab go through a weeklong hospital orientation, including skills training, and are then oriented to the cath lab for 6 weeks to 3 months, depending on the first role. Our cath lab is continuously training and orienting to new procedures, skills, and roles, so the training really never stops.
Like many cath labs, Sheridan’s cath lab receives continuing education through vendor support and training days. We also partner with regional medical centers in the region for cardiac-specific educational opportunities. SMH also subscribes to HealthNet (Texas Tech University Health Sciences Center) for online continuing educational credit. We take every opportunity to learn and advance our practice and experience.
Vendors reserve appointments through the cath lab manager and are placed on our schedule in order to ensure that there are no concerns or conflicts. When vendor representatives arrive, they must check in via our RepTrak system and arrive to the lab immediately.
Staff has a yearly competency that coincides with their evaluation. We also have a skills fair every July, where we use high-fidelity simulation in the lab for high-risk, low-volume procedures. Last year, our focus was on insertion and transport of a patient on an IABP to the regional medical center two hours away. This included our local EMS transporting the “patient” from the cath lab table to the ambulance, and then to the airport for a simulated fixed-wing transport to our regional medical center for CABG. We decided to perform this full-transport training to work out positioning issues within the ambulance and fixed-wing planes.
At this time, our cath lab does not have a clinical ladder specific to the department; however, each team member has specific professional goals that they have set to increase their growth in the organization. The hospital does have a clinical ladder called the Professional Incentive Program (formally known as the Clinical Ladder Program), which is available for all RNs, LPNs, surgical techs, CNAs and unit coordinators. There is no clinical ladder for RTs at this time.
Our cath lab call team consists of the same mix of staff as any other case; we must always have one RN for sedation, but the scrub and monitor roles can be performed by either RN or RT, as long as they have been oriented, trained, and checked off for STEMI compliance for the role. There are many times when the cardiologist is assisted with one RN and two RTs.
Our call team is expected to be ready to assume care of the patient 30 minutes after being paged, meaning at 30 minutes the team has arrived, supplies are available, and the table is set up.
The cath lab schedule usually consists of two shift start times. If the team member is on call, then the start time is 0700; if the team member is not on call, then they have an 0800 start time. Some of the team members have made a pact that they will always be available at 0700. All shifts are scheduled for eight-hour shifts, but the team understands that there may be opportunity to leave early or stay late, depending on the caseload and patient needs.
Yes, our cath lab recently underwent certification by The Joint Commission. The auditor spent two days going over our processes, policies and practices, and we were found to have no issues. We are very proud of this first visit, and look forward to the opportunities and education from future visits.
The cath lab is located on the ground floor of the hospital, and the STEMI doors are located approximately 50 feet from the trauma rooms of our ED. We were strategically placed between the ED trauma rooms, radiology, surgery, and the ICU. There is no more than a two-minute transport time from either cath lab room to any of the three other departments.
Our cath lab was designed by Mark Averett (TSP, Sheridan, Wyoming), who specializes in healthcare architecture. The best feature of our layout includes the STEMI doors within feet of the trauma bay area of the ED, which is where STEMIs are taken upon arrival to the hospital.
Because the architecture firm was integrating into a first story area of the hospital for one of the labs, we were not able to mirror the large screen display for our STEMI room. It would have been perfect if we could have the large screens in both labs.
At this time, we are still taking data points for trending purposes. Recent AHA data shows that the state of Wyoming, as a whole, continues to trend closely with national data. Our typical STEMI patients are 60- to 65-year-old males. The cath lab, hospital administrators and community leaders have been working closely to develop public service announcement and community awareness of cardiac disease in both men and women, and the use of 911 at the first sign of a heart attack.
Our cath lab was only the third cath lab built in the state of Wyoming when we opened. As stated before, due to our location within the hospital, we have a two-minute or less transport time to the ED, ICU, and surgery.
There are two challenges that Sheridan’s cath lab faces. Like any rural hospital, we are challenged with getting the right mix of personalities for staffing. Wyoming has a significant nursing shortage and we are no exception. To try to circumvent this issue, we always try to market the cath lab as a great specialty for students and new nurses, and keep in contact with our partners throughout Wyoming and Montana for staffing opportunities.
Our cath lab staff members are not required to sit for the RCIS certification at this time; however, they are all encouraged to move forward on educational opportunities and certifications. With the new caseload requirements for RCIS, each team member has a while before we hit the 600 case requirements.

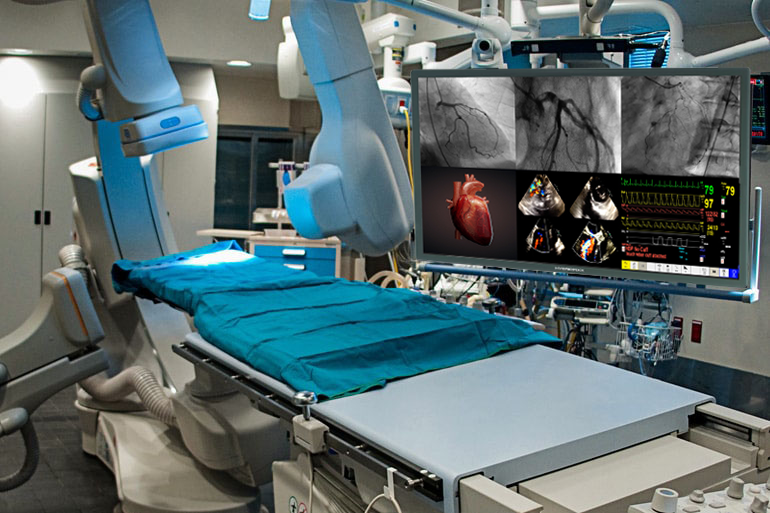
Cath lab operations depend completely upon medical displays, which allow physicians to visualize a patient internally and perform the necessary procedure. The digital age has ushered in improved imaging technologies, which emit less radiation and also provide greater visual clarity to physicians. The adoption of CRT monitors in the cath lab brought about significant changes in their operations. CRT displays were followed by the advent of LCD screens. Most hospitals and healthcare facilities upgraded to LCD screens as they are slimmer, portable and offer higher resolution images. Currently, cath labs are witnessing yet another transition in medical monitors, as professionals are upgrading from LED displays to ultra-high definition 4K technology. Instead of using four to six displays, hospitals and healthcare facilities are upgrading to one large UHD 4K display. However, healthcare providers need to consider several variables before deciding upon the kind of upgrades they can make. Additionally, the switch from the LED model to the 4K display system introduces issues related to maintenance and safety.
Ampronix (Irvine, CA, USA), an authorized master distributor of the medical industry"s top brands and a manufacturer of innovative technology, has been repairing and selling 4K monitors of different sizes for cath labs and hybrid ORs to hospitals for years. Ampronix undertakes sale, service and repair of cath lab monitors manufactured by several well-known companies such as Philips, GE, Siemens, Shimadzu, Toshiba, Hitachi, Eizo, Barco, Chilin and Optik View. Ampronix offers tailored, one-stop solutions at a faster and more cost effective rate than other manufacturers. The company has most models in stock that are available at half the OEM price.
The company’s services also include preventive maintenance, replacement of LCD, backlights, reflectors and power supplies. Any display failure amounts to an entire cath lab rendered obsolete until a replacement or repair solution is provided. However, the turnaround time for either of those protocols can be several weeks. Given the importance of the cath lab for healthcare providers, Ampronix ensures that they have zero downtime in the event of their monitors requiring service or replacement. The company has a readily available response team of ESD- and ASQ-certified technicians to assist and answer questions for urgent repairs. Nation-wide requests received by 2pm PST receive same-day or next-day delivery. Ampronix also has capable and competent customer service representatives for addressing all medical technology questions and concerns. With its extensive product knowledge, outstanding service, and state-of-the-art repair facility, Ampronix continues to meet the needs of the medical community and move forward with its goal to facilitate optimized patient care and improved physician workflow.

In the control room, clinical staff can monitor all patient vital signs, analyze physiological parameters and easily display calculation results in the exam room. Results are displayed as a numerical value and a gradient image. Displaying numerical and graphical results helps clinical staff stay focused on the tasks at hand without the need to leave the sterile area.
In the control room, clinical staff can monitor all patient vital signs, analyze physiological parameters and easily display calculation results in the exam room. Results are displayed as a numerical value and a gradient image. Displaying numerical and graphical results helps clinical staff stay focused on the tasks at hand without the need to leave the sterile area.
In the control room, clinical staff can monitor all patient vital signs, analyze physiological parameters and easily display calculation results in the exam room. Results are displayed as a numerical value and a gradient image. Displaying numerical and graphical results helps clinical staff stay focused on the tasks at hand without the need to leave the sterile area.
In the control room, clinical staff can monitor all patient vital signs, analyze physiological parameters and easily display calculation results in the exam room. Results are displayed as a numerical value and a gradient image. Displaying numerical and graphical results helps clinical staff stay focused on the tasks at hand without the need to leave the sterile area.
The new user interface provides on-screen guidance to help team members smoothly proceed through procedures and work efficiently with each other. The workstation"s interactive heart diagram aids team members in the control room in quickly performing pullbacks and changing the pressure labels. These features promote ease of use by all staff members with minimal training.
The new user interface provides on-screen guidance to help team members smoothly proceed through procedures and work efficiently with each other. The workstation"s interactive heart diagram aids team members in the control room in quickly performing pullbacks and changing the pressure labels. These features promote ease of use by all staff members with minimal training.
The new user interface provides on-screen guidance to help team members smoothly proceed through procedures and work efficiently with each other. The workstation"s interactive heart diagram aids team members in the control room in quickly performing pullbacks and changing the pressure labels. These features promote ease of use by all staff members with minimal training.
The new user interface provides on-screen guidance to help team members smoothly proceed through procedures and work efficiently with each other. The workstation"s interactive heart diagram aids team members in the control room in quickly performing pullbacks and changing the pressure labels. These features promote ease of use by all staff members with minimal training.
Choose from a variety of configurations of the Interventional Hemodynamic System. Each system comes with a patient monitoring device mounted at the table side. Single and dual configurations of the workstation are available. With the dual display configuration in the control room you can always view patient monitoring, hemodynamic analyses and reports on a full screen.
Choose from a variety of configurations of the Interventional Hemodynamic System. Each system comes with a patient monitoring device mounted at the table side. Single and dual configurations of the workstation are available. With the dual display configuration in the control room you can always view patient monitoring, hemodynamic analyses and reports on a full screen.
Choose from a variety of configurations of the Interventional Hemodynamic System. Each system comes with a patient monitoring device mounted at the table side. Single and dual configurations of the workstation are available. With the dual display configuration in the control room you can always view patient monitoring, hemodynamic analyses and reports on a full screen.
Choose from a variety of configurations of the Interventional Hemodynamic System. Each system comes with a patient monitoring device mounted at the table side. Single and dual configurations of the workstation are available. With the dual display configuration in the control room you can always view patient monitoring, hemodynamic analyses and reports on a full screen.
Each system comes with a IntelliVue X3 a compact patient monitor. When mounted at the table in the cathlab, you have unrestricted access to your patient from nearly any position, without restricting table movement. It’s small enough to hold in your hands and can be easily mounted where you need it most.
Each system comes with a IntelliVue X3 a compact patient monitor. When mounted at the table in the cathlab, you have unrestricted access to your patient from nearly any position, without restricting table movement. It’s small enough to hold in your hands and can be easily mounted where you need it most.
Each system comes with a IntelliVue X3 a compact patient monitor. When mounted at the table in the cathlab, you have unrestricted access to your patient from nearly any position, without restricting table movement. It’s small enough to hold in your hands and can be easily mounted where you need it most.
Each system comes with a IntelliVue X3 a compact patient monitor. When mounted at the table in the cathlab, you have unrestricted access to your patient from nearly any position, without restricting table movement. It’s small enough to hold in your hands and can be easily mounted where you need it most.
The fully integrated functional measurement option allows you to perform and analyze instant wave-free Ratio (iFR) Spot and Scout pullback measurement in both the exam and control room. This is your gateway to bring the latest hemodynamic monitoring and physiological techniques into the interventional lab.
The fully integrated functional measurement option allows you to perform and analyze instant wave-free Ratio (iFR) Spot and Scout pullback measurement in both the exam and control room. This is your gateway to bring the latest hemodynamic monitoring and physiological techniques into the interventional lab.
The fully integrated functional measurement option allows you to perform and analyze instant wave-free Ratio (iFR) Spot and Scout pullback measurement in both the exam and control room. This is your gateway to bring the latest hemodynamic monitoring and physiological techniques into the interventional lab.
The fully integrated functional measurement option allows you to perform and analyze instant wave-free Ratio (iFR) Spot and Scout pullback measurement in both the exam and control room. This is your gateway to bring the latest hemodynamic monitoring and physiological techniques into the interventional lab.
By connecting the IntelliVue X3 in the cath lab with the Philips Hemo system, you can continuously monitor a patient. There is no need to change cables, minimizing disruption and giving you more time to focus on your patient.
By connecting the IntelliVue X3 in the cath lab with the Philips Hemo system, you can continuously monitor a patient. There is no need to change cables, minimizing disruption and giving you more time to focus on your patient.
By connecting the IntelliVue X3 in the cath lab with the Philips Hemo system, you can continuously monitor a patient. There is no need to change cables, minimizing disruption and giving you more time to focus on your patient.
By connecting the IntelliVue X3 in the cath lab with the Philips Hemo system, you can continuously monitor a patient. There is no need to change cables, minimizing disruption and giving you more time to focus on your patient.

Please select Acre Agrigento Alabama Alagoas Alaska Alberta Alessandria Amapá Amazonas Amazonas Ancona Andaman and Nicobar Islands Andhra Pradesh Anhui Antioquia Aosta Arauca Arezzo Arizona Arkansas Arunāchal Pradesh Ascoli Piceno Assam Asti Atlántico Australian Capital Territory Avellino Bahia Bari Barletta-Andria-Trani Beijing Belluno Benevento Bergamo Biella Bihār Bogotá Bologna Bolzano Bolívar Boyacá Brescia Brindisi British Columbia Cagliari Caldas California Caltanissetta Campobasso Caquetá Carbonia-Iglesias Casanare Caserta Catania Catanzaro Ceará Cesar Chandīgarh Chhattīsgarh Chieti Chocó Chongqing Colorado Como Connecticut Cosenza Cremona Crotone Cundinamarca Cuneo Córdoba Damān and Diu Delaware Delhi District of Columbia Distrito Federal Dādra and Nagar Haveli Enna Espírito Santo Fermo Ferrara Firenze Florida Foggia Forli Forli-Cesena Frosinone Fujian Gansu Genova Georgia Goa Goiás Gorizia Grosseto Guainía Guangdong Guangxi Guaviare Guizhou Gujarāt Hainan Haryāna Hawaii Hebei Heilongjiang Henan Himāchal Pradesh Hubei Huila Hunan Idaho Illinois Imperia Indiana Iowa Isernia Jammu and Kashmīr Jharkhand Jiangsu Jiangxi Jilin Kansas Karnātaka Kentucky Kerala L"Aquila La Guajira La Spezia Lakshadweep Latina Lecce Lecco Liaoning Livorno Lodi Louisiana Lucca Macerata Madhya Pradesh Magdalena Mahārāshtra Maine Manipur Manitoba Mantova Maranhão Maryland Massa-Carrara Massachusetts Matera Mato Grosso Mato Grosso do Sul Medio Campidano Meghālaya Messina Meta Michigan Milano Minas Gerais Minnesota Mississippi Missouri Mizoram Modena Montana Monza e Brianza Napoli Nariño Nebraska Nei Mongol Nevada New Brunswick New Hampshire New Jersey New Mexico New South Wales New York Newfoundland and Labrador Ningxia Norte de Santander North Carolina North Dakota Northern Territory Northwest Territories Nova Scotia Novara Nunavut Nuoro Nāgāland Ogliastra Ohio Oklahoma Olbia-Tempio Ontario Oregon Orissa Oristano Padova Palermo Paraná Paraíba Parma Pará Pavia Pennsylvania Pernambuco Perugia Pesaro e Urbino Pescara Piacenza Piauí Pisa Pistoia Pondicherry Pordenone Potenza Prato Prince Edward Island Punjab Putumayo Qinghai Quebec Queensland Quindío Ragusa Ravenna Reggio Calabria Reggio Emilia Rhode Island Rieti Rimini Rio Grande do Norte Rio Grande do Sul Rio de Janeiro Risaralda Roma Rondônia Roraima Rovigo Rājasthān Salerno San Andrésy Providencia Santa Catarina Santander Saskatchewan Sassari Savona Sergipe Shaanxi Shandong Shanghai Shanxi Sichuan Siena Sikkim Siracusa Sondrio South Australia South Carolina South Dakota Sucre São Paulo Tamil Nādu Taranto Tasmania Telangana Tennessee Teramo Terni Texas Tianjin Tocantins Tolima Torino Trapani Trento Treviso Trieste Tripura Udine Utah Uttar Pradesh Uttarakhand Valledel Cauca Varese Vaupés Venezia Verbano-Cusio-Ossola Vercelli Vermont Verona Vibo Valentia Vicenza Vichada Victoria Virginia Viterbo Washington West Bengal West Virginia Western Australia Wisconsin Wyoming Xinjiang Xizang Yukon Territory Yunnan Zhejiang

There have been tremendous advances in 3-dimensional (3-D) technologies in the past few years, not only in various medical and surgical fields but also in our daily lives outside of work; with more and more new features in cell phones, computer design programs, and movies!! 4-dimensional (4-D) imaging captures 3-D images over time. These technologies are particularly important in cardiology, especially in interventional cardiology. The heart is a very dynamic organ, and understanding the variation in the anatomy of vessels and geometry of cardiac structures is key to ensuring successful procedures, patient’s safety and good outcomes. More recently, newer innovations in both 3-D and 4-D technologies have been developed, so I decided to shed light on some of these innovations and how they can be potential game-changers in the cath lab.
This technology was actually displayed at the Transcatheter Cardiovascular Therapeutics (TCT) 2019 meeting. It converts live transesophageal echo (TEE) imaging into real-time 3-D holographic video in the cath lab to aid structural heart procedures. The 3-D hologram is projected on a special display screen, and the interventional cardiologist uses hand movements and a foot pedal/switch to change the image orientation without breaking the sterile field. It also allows the operator to see the tools they use in the cath lab, including catheters or devices, in real-time in a 3-D format. This technology does not even require the user to wear 3-D glasses! It was submitted for FDA regulatory review in September 2019.
In conclusion, we have seen and continue to see tremendous advances in the innovations of 3-D and 4-D imaging with important implications in our work in the cath lab. With our continued collaboration with informational technology experts, engineers, and scientists, these innovations are potentially game-changers in different fields, including coronary interventions and structural heart procedures. I look forward to seeing how this technology continues to evolve in the coming decades!!

Cardiologists use a procedure called cardiac catheterization to see how well your heart is working. It can also be used to identify problems and administer a treatment for narrowed or blocked coronary arteries.
A cardiac catheterization (sometimes referred to as a “cardiac cath” or a “heart catheterization”) is a procedure that measures the pressure and blood flow in and around the heart. It can also be used to treat certain heart conditions.
Cardiac catheterizations are performed by a specially-trained doctor and a team of nurses and technicians in a hospital’s cardiac catheterization (cath) lab.
When it’s time for the procedure, a nurse will put an IV line into your arm to administer a sedative. You’ll feel relaxed during the procedure, but you’ll be awake and able to follow instructions. A nurse will also clean and shave the area where the catheter will be inserted (usually the wrist, groin or neck) and use a local anesthetic to numb the area.
Your doctor will insert a small tube called a sheath into a vein or artery. Then, they will gently guide an even smaller tube called a catheter into the blood vessel through the sheath. A video screen will display the catheter’s position as it goes through the major blood vessels to the heart. You may feel pressure, but you shouldn’t experience any pain.
The catheter may also be used to inject contrast dye so that the doctor can create X-rays of your heart’s valves, chambers, and coronary arteries. This test is called an angiography.
While a cardiac catheterization usually takes about 30 minutes, the preparation and recovery time add several hours. You should plan on being at the hospital all day, and make sure someone is able to drive you home after the procedure.
You’ll be given instructions about what you can eat and drink during the 24 hours prior to your cardiac catheterization. Typically, you’ll be asked to not eat or drink anything for six to eight hours beforehand.
Your doctor will want to know about any medications you’re taking, including over-the-counter vitamins and supplements. They may ask you to not take them prior to your cardiac catheterization; don’t stop taking them before you’re instructed to do so.
After the procedure, you’ll be moved to a recovery room where you’ll lie flat for a few hours if the catheterization was done via the groin. If the catheter was inserted through your groin, you’ll be asked to keep the closest leg straight. If the catheterization was performed from the wrist or from the neck, you will be observed in the recovery area but can sit up.
Most people can return to their normal activities the day after the procedure, though you’ll want to avoid strenuous exercise and lifting heavy objects for two weeks. Some additional time may be needed if a treatment was done during your cardiac catheterization. Your doctor will advise you accordingly.
Cardiac catheterization is generally a safe procedure. Some people experience minor issues, like bruising around the area where the catheter was inserted. Others may have an allergic reaction to the contrast dye, which can cause nausea.
A catheterization laboratory, commonly referred to as a cath lab, is a procedural room in a hospital or clinic with diagnostic imaging equipment used to visualize the arteries during procedures. Cath labs house procedural machines that assists in the imaging processes during heart catheterizations and other cardiac procedures like pace maker placement, or placement of filters for blood clots.
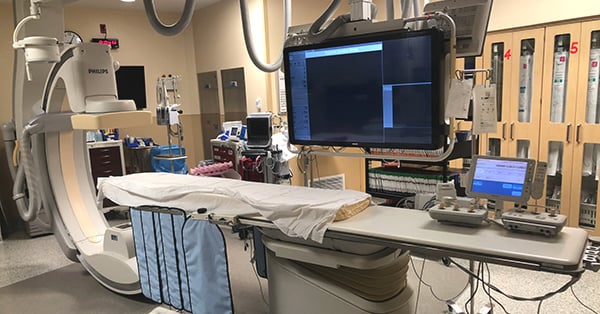
The cath lab at UH Samaritan was built back in 2002 and the equipment was all original to the opening of this department. Recently, there were upgrades made in order to provide better images during procedures with less radiation exposure for both patients and staff. These changes will improve patient outcomes and patient safety. The cath lab at UH Samaritan was able to install a Philips Azurion system. Images from the Azurion system show on a large screen so doctors have a high quality view as they complete each procedure.
Currently, UH Samaritan is a Level 1 cath lab, which means we are a diagnostic cath lab. These types of catheterizations are normally done for clearance for more complicated procedures or patients that have a low risk for any blockage in the heart. UH Samaritans cath lab allows Dr. Yulanka Castro- Dominguez, MD, a UH Samaritan cardiologist, to perform procedures on vessels on both the right and left sides of the heart. Dr. Castro also uses the new technology to place stents to open the vessels in the legs allowing the patients to get better blood flow to their lower extremities.
With the upgrades to the cath lab we can now offer electrophysiology treatment, or EP, at UH Samaritan. Dr. Shashank Jain, MD, a cardiologist who specializes in electrophysiology uses the cath lab for these procedures. EP has to do with the function of the electrical system within the heart. Dr. Jain uses EP treatment for patients with conditions like atrial fibrillation and other conditions that affect the electrical function of the heart. Dr. Jain will use the new technologies to implant pace makers that help maintain regular electrical activity in the heart and loop recorders, a device that records the information about the electrical activity in the heart.
Dr. Young, DO, a nephrologist and intensive care doctor at UH Samaritan, will also utilize the upgrades to the cath lab. Dr. Young uses the cath lab and its new technologies to place dialysis catheters in patients who need dialysis treatment because their kidneys can no longer effectively filter toxins from their blood.
What does having this upgraded cath lab mean to the Ashland community and those who have access to UH Samaritan? According to Jordan Repp, RN, the cath lab clinical coordinator at UH Samaritan, the new technologies are a great resource for our local community and surrounding areas. It will provide a chance for our patients to get the best care and treatment that University Hospitals has to offer while staying close to home. Folks will have fewer transportation concerns and less worry about the need for transfer to other hospitals because they can receive the treatment they need right at UH Samaritan.
What are the long-term goals for the cath lab at UH Samaritan? The future is bright here at UH Samarian Medical Center, says Jordan. Like previously mentioned, UH Samaritan is a level 1 cath lab, we are working toward becoming a level 2 cath lab. This means that we will be able to perform catheterizations to place stents inside the arteries of the heart to eliminate blockages. As a level 2 cath lab, when a patient comes in having a heart attack we will be able to treat these patients here and not have to transfer them. Time is muscle, which means the faster we can get them to the cath lab and open up the blockage the better the heart is going to respond. Clearly, this goal will be beneficial to people with access to UH Samaritan Medical Center.
Join us on Tuesday, Aug. 23, 2022 from 4:30 to 6:30 p.m. for an open house to celebrate the cath lab upgrades at University Hospitals Samaritan Medical Center. You will have the chance to tour the cath lab, learn about the new technologies and services provided, as well as meet the doctors who will utilize the new state of the art equipment during procedures.



 Ms.Josey
Ms.Josey 
 Ms.Josey
Ms.Josey